
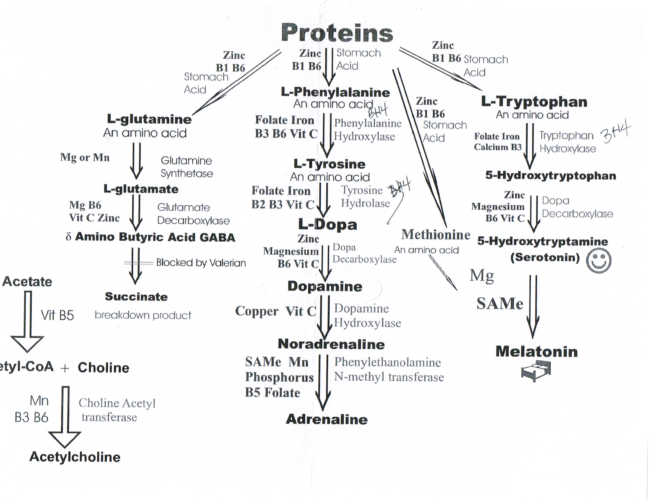
I have suspected for years that b6 deficiency may be a significant contributer to multiple metabolic disorders that I’ve come across frequently in my practice. B6 is a critical nutrient for nerve conductivity, the synthesis of neurotransmitters and serves as a critical cofactor in multiple functions of the body including glucose metabolism, amino acid conversions and lipids (fats) utilization. Below is one of my favorite charts of reference that I may discuss with my clients showing the critical importance of B6. It serves to support conversions from food into the GABA conversion(calming amino acid), into seretonin and melatonin pathways, into autonomic nervous system neurotransmitters (noradrenaline and acetylcholine) and so much more!
How do we know the status of B6? Rather than a guess I test using an organic acids test or a NutrEval. However, based on my clinical experiences for more than 10 years I’ve observed b6 deficiency in nearly every one of my clients. My research below over the years has reflected the necessity for b6 as a critical nutrient to support high oxalates, GABA production, pyroluria, pyridoxine deficiency, general nutritional deficiencies, sleep (dream recall is a good gauge), focus, reduction in anxiety, and so much more. Here are a few articles I’ve written with regards to b6 optimal supplementation.
B6 deficiency may lead to oxalates.
GABA production requires optimal levels of b6
Pyroluria, Seizures and the need for b6
Bioavailable B6 and the cessation of seizures even in youth
To no surprise, I’ve recently come across this article Seizures related to Vitamin B6 Deficiency in Adults. Per the findings:
“Vitamin B6 is closely associated with functions of the nervous, immune, and endocrine systems. Its deficiency may result in neurological disorders including convulsions and epileptic encephalopathy. Until today, this has only been reported in infants, children, and critically ill adult patients. We report a case of a 36year-old man with chronic alcoholism who presented with seizures after gastrointestinal disturbance. His seizures persisted even after treatment with antiepileptic drugs, but eventually disappeared after administration of pyridoxine. Hence, vitamin B6 deficiency may cause seizures in adult patients with chronic alcoholism.”
It refers to vitamin b6 deficiency and its cause for seizures. The reference of how the patient became deficient in b6 is through alcoholism. However, I find this relevant and not relevant. There are varying reasons that a person can become deficient in b6. In my field I find that most of my clients fall under one or more of the areas below. Here are a few:
- Malnutrition
- Restricted diets
- Food processing
- Malabsorption: celiac, crohn’s disease, IBD
- Kidney dysfunction
- Liver dysfunction
- Antiepileptic drugs
- Autoimmunity, etc
Many of my clients will explain that they are taking some form of b6 at the time of providing a lab sample. When we work together I closely examine: the results of all lab tests, the current dosing and intake and type of b6 (pyridoxine hcl or P5P). The client’s age, potential immune dysregulation, sensitivity to changes, the areas of healing identified and their health history are all factored into my recommendation of b6 type and dosing. For example, a recent client I worked with was 6 years of age, taking antiepileptic drugs, reported ongoing digestive issues, suspected glutamate toxicity and lab results indicated elevated kryptopyrolles. ALL of these findings indicated a b6 deficiency and warranted a hyper focus on the type of b6 to consume and the dosing. This dosing recommendation was significantly higher than a client I had worked with earlier that day. In other words, b6 dosing is NOT a one size fits all, it is NOT based strictly on age and it almost always involves much higher dosing than the recommended daily allowance. Consult a qualified practitioner.
Much light,
Lynn

